May 15, 2022 Analysis of US state data
This report shows the result of analyses that use hospital admission data to estimate the transmission rates in the past few months to characterize the BA.1 and BA.2 Omicron strains. The only parameters adjusted are the transmission rates and normalization constants. Hospital admission data are used, to avoid testing capacity issues and to better predict future hospital admission rates.
The Omicron variants are assumed to have a much larger susceptible population, due to its ability to evade immunity (natural and vaccination immunity). For this study, those immunized against earlier strains only have 20% effective immunity against omicron.
Booster doses have been included in this analysis, and are assumed to raise the vaccine effectiveness from 20% to 80% with a time delay given by a gamma distribution with mean 10 days and standard deviation 5 days. The Omicron variants are also assumed to produce more infections that go undetected as cases (as compard to Delta).
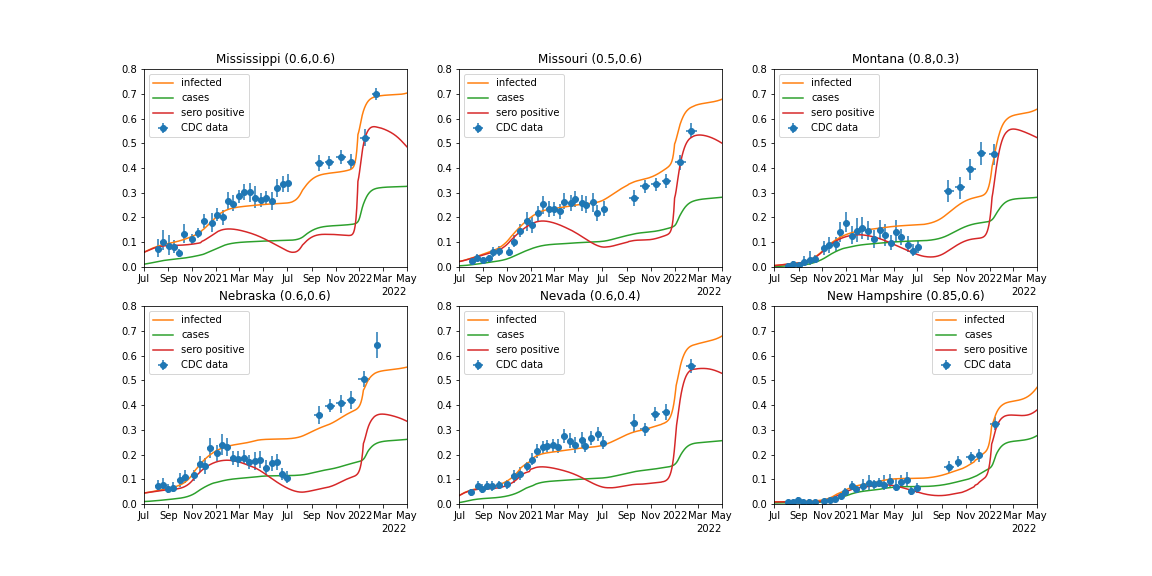
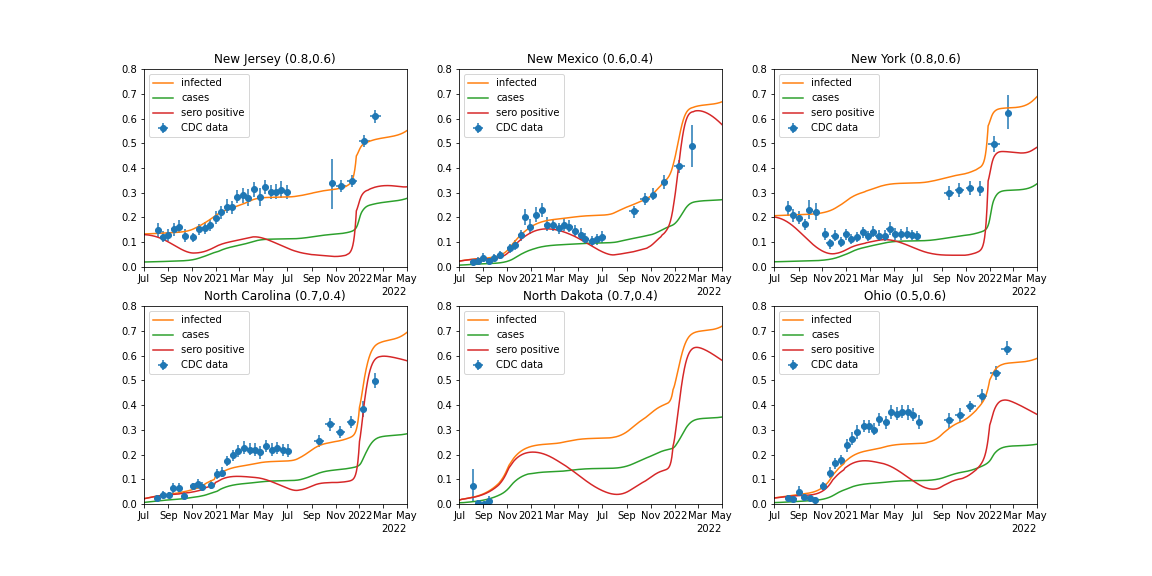
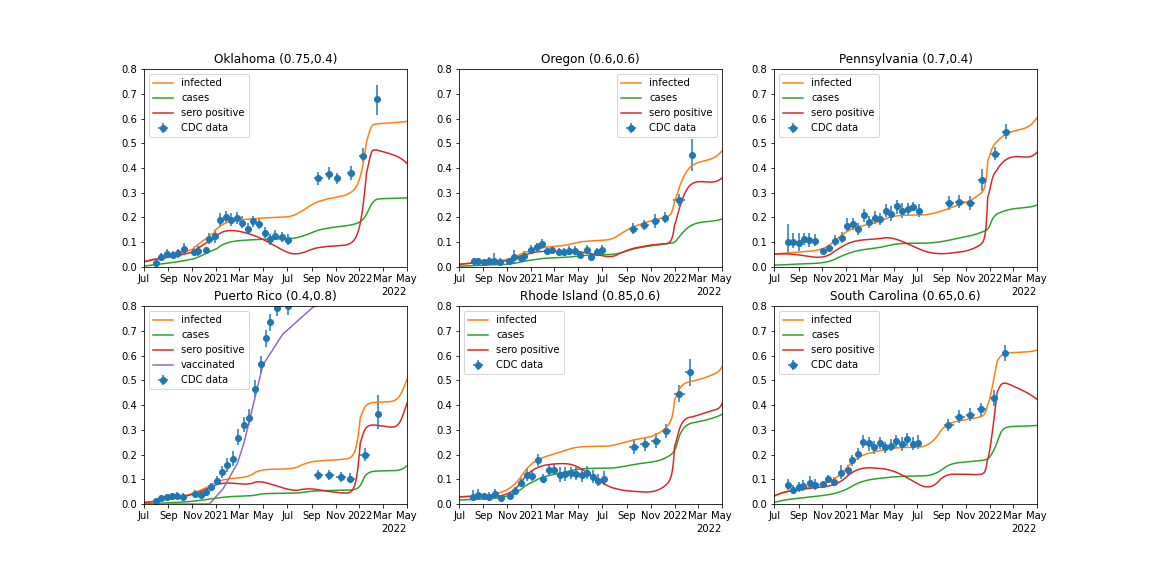
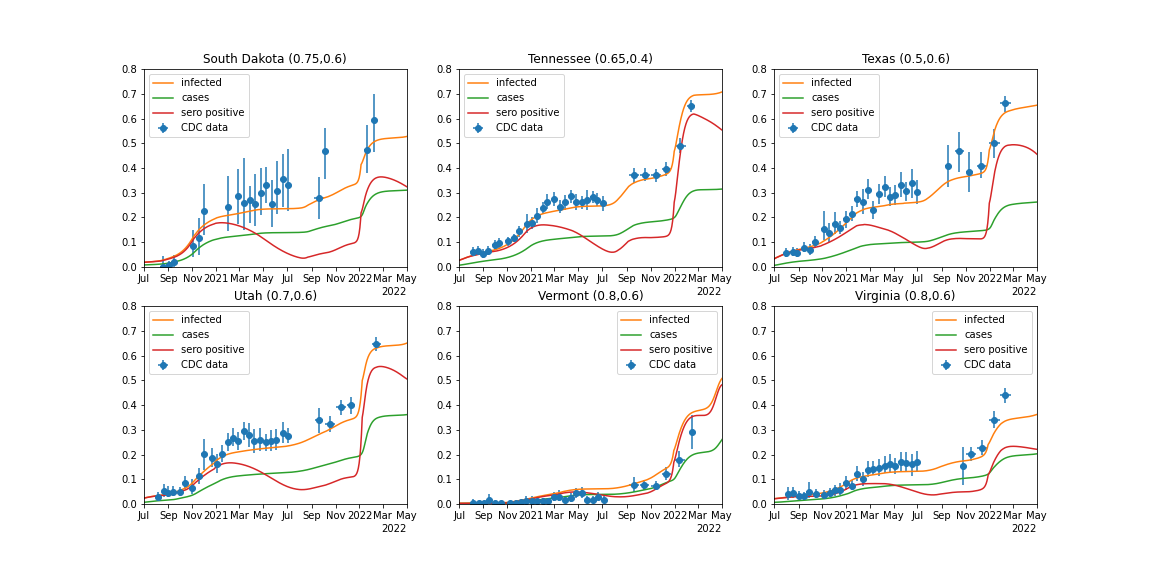
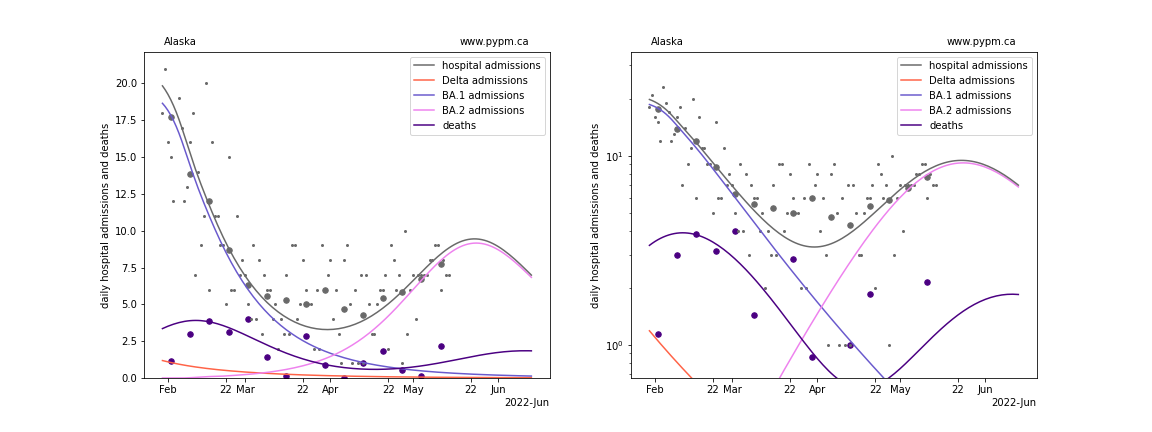
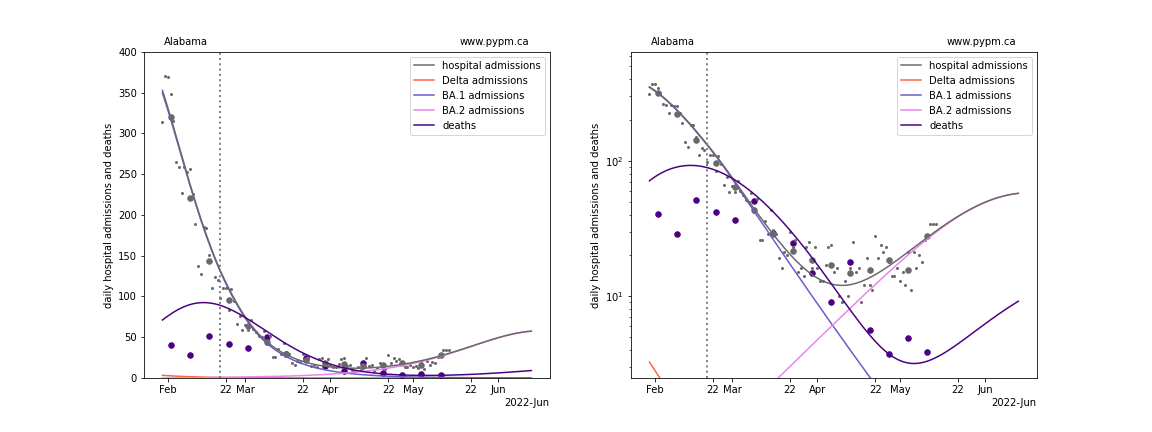
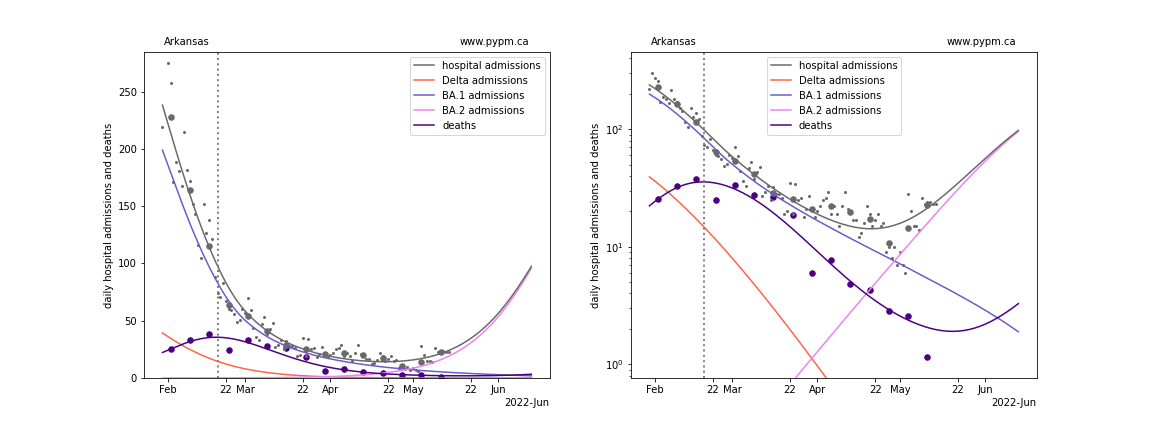
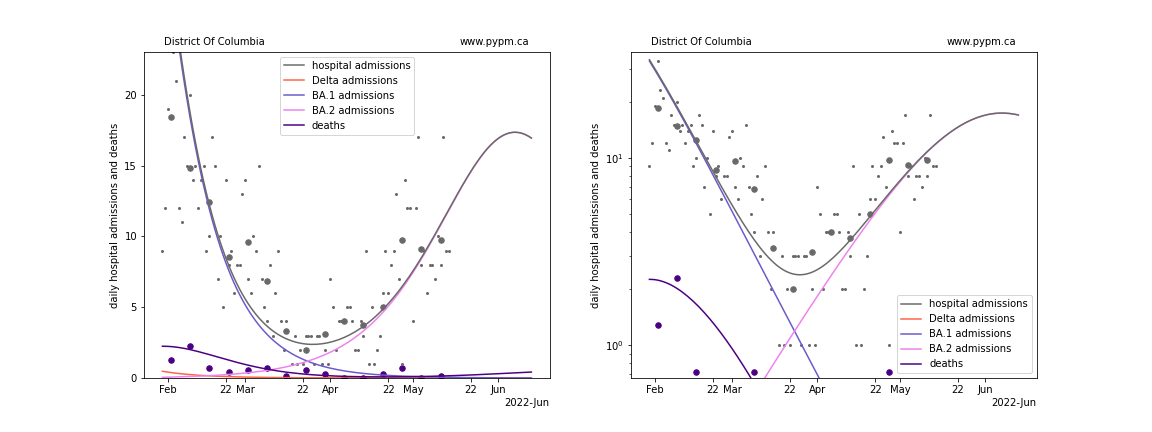
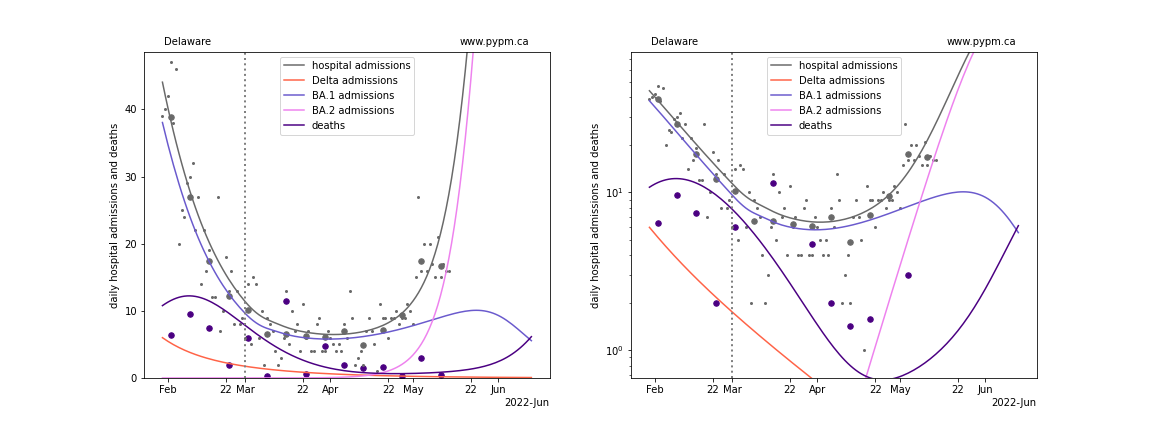
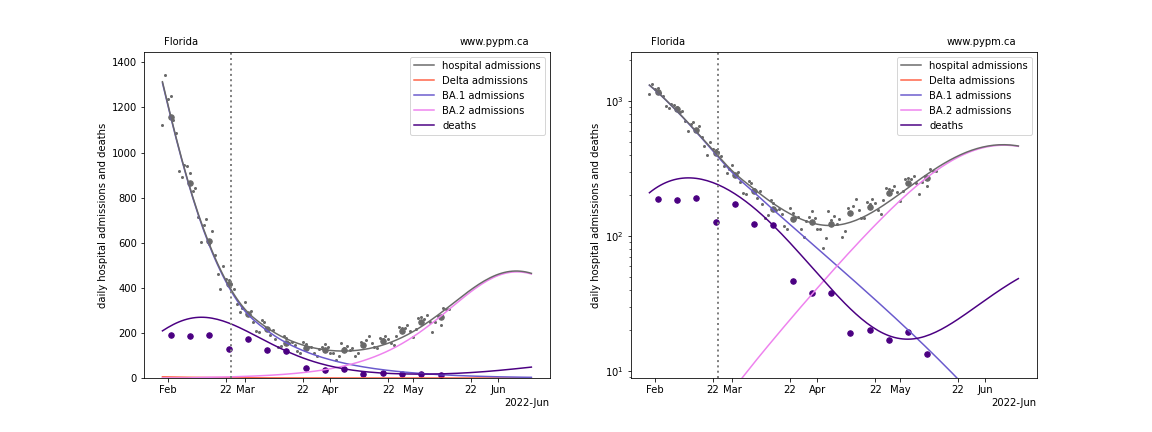
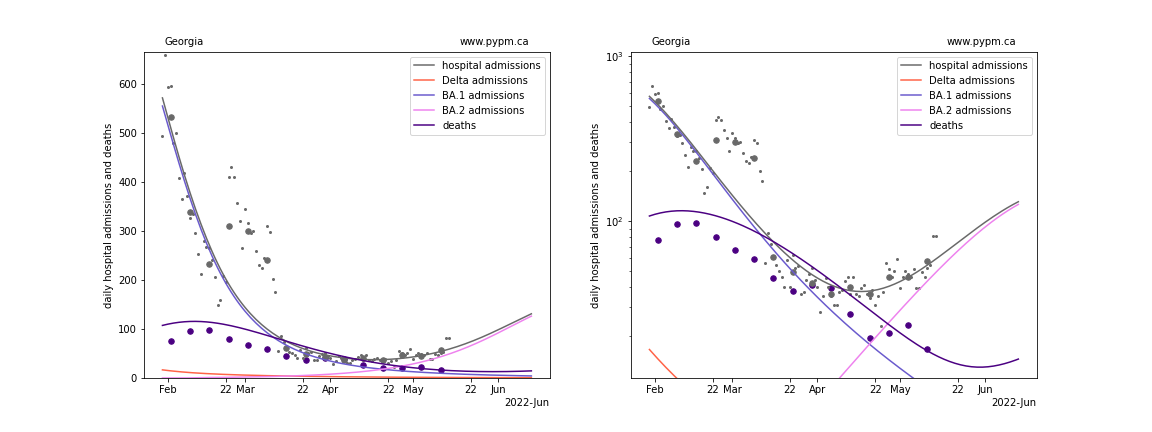
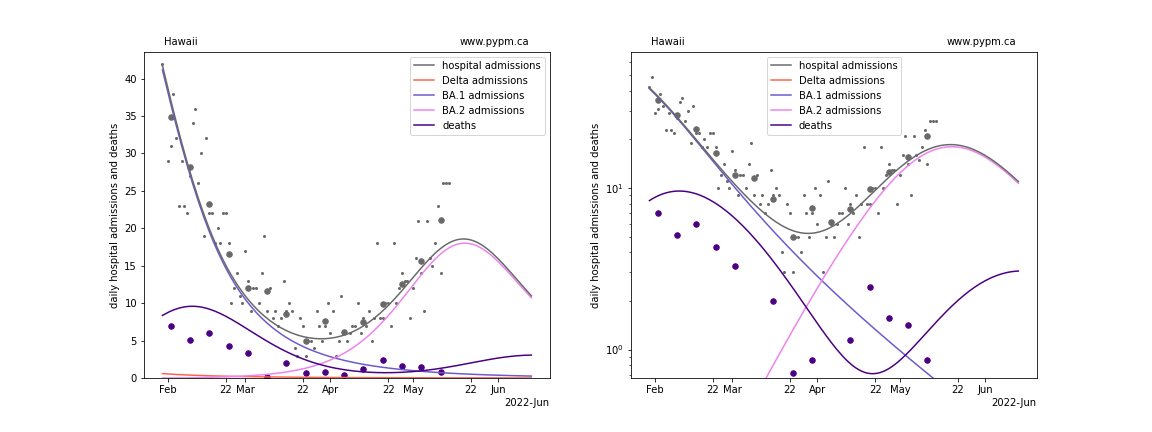
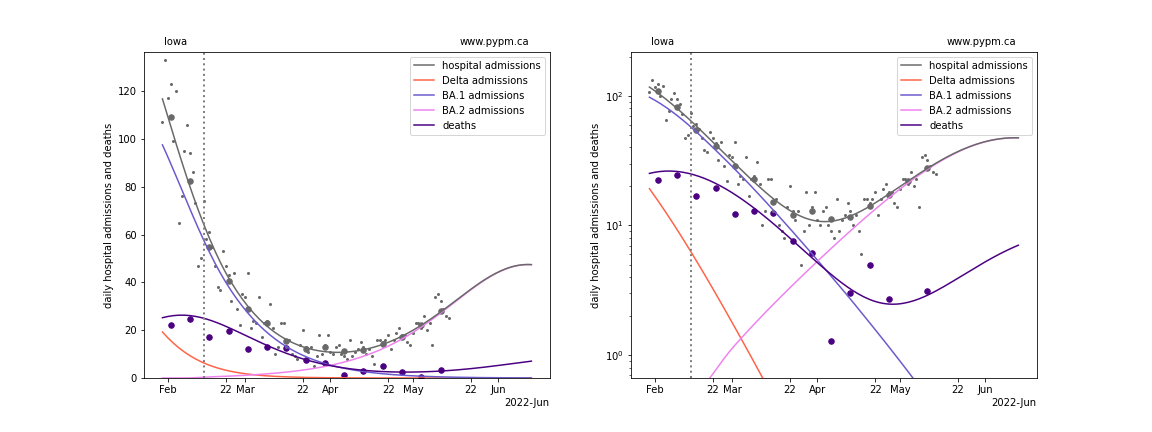
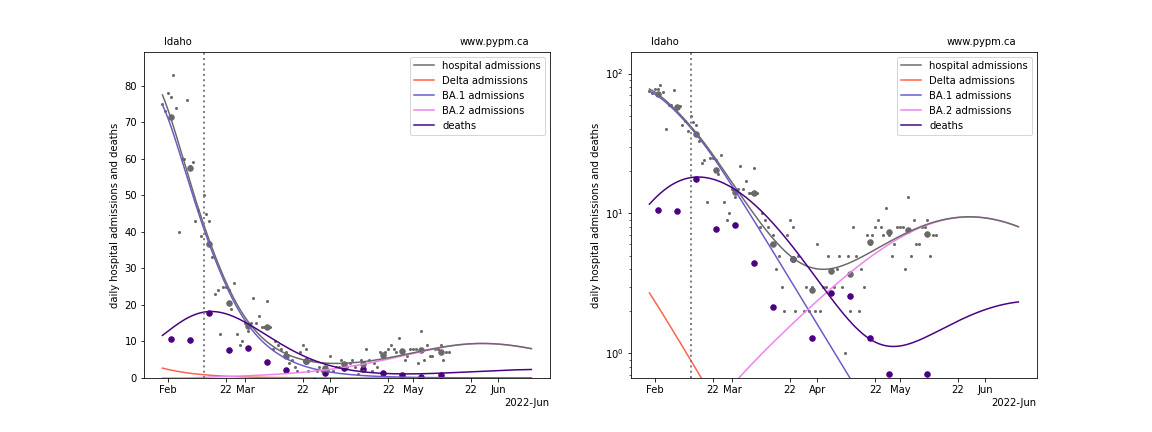
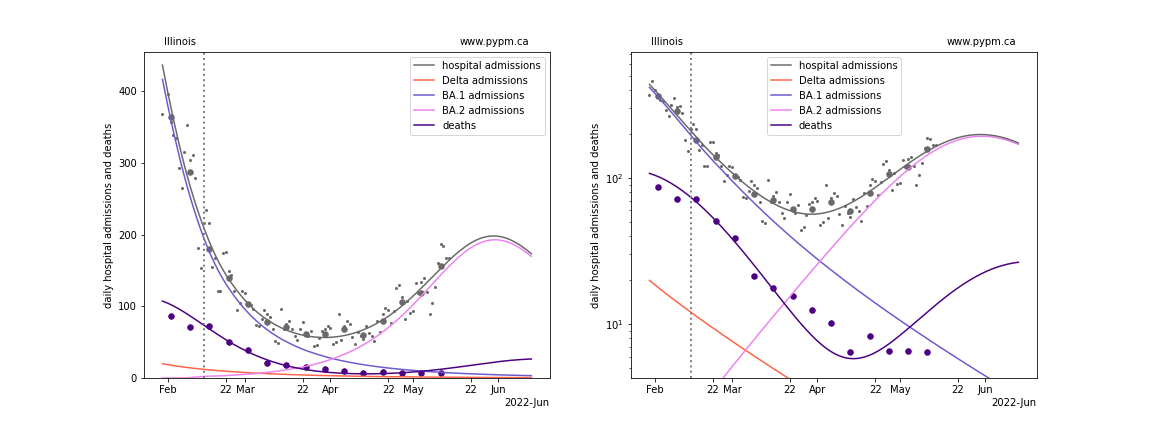
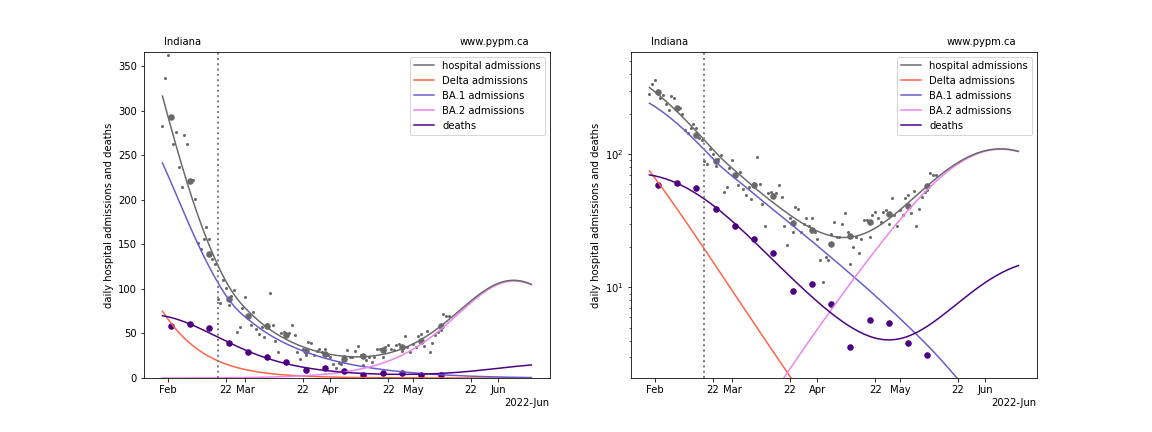
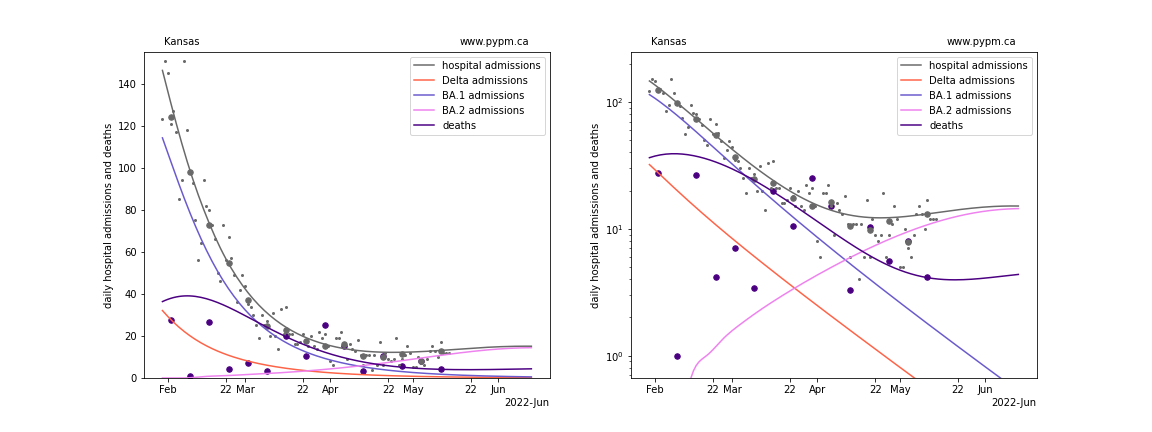
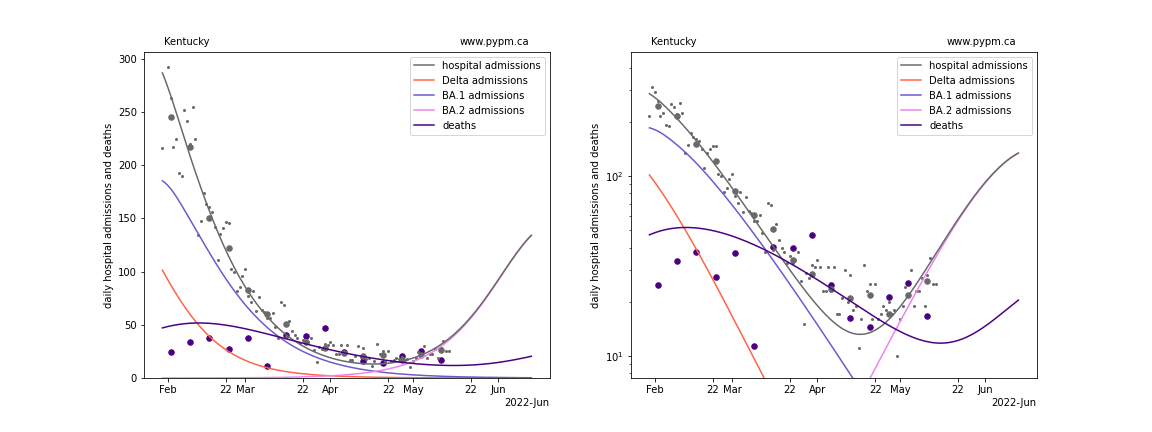
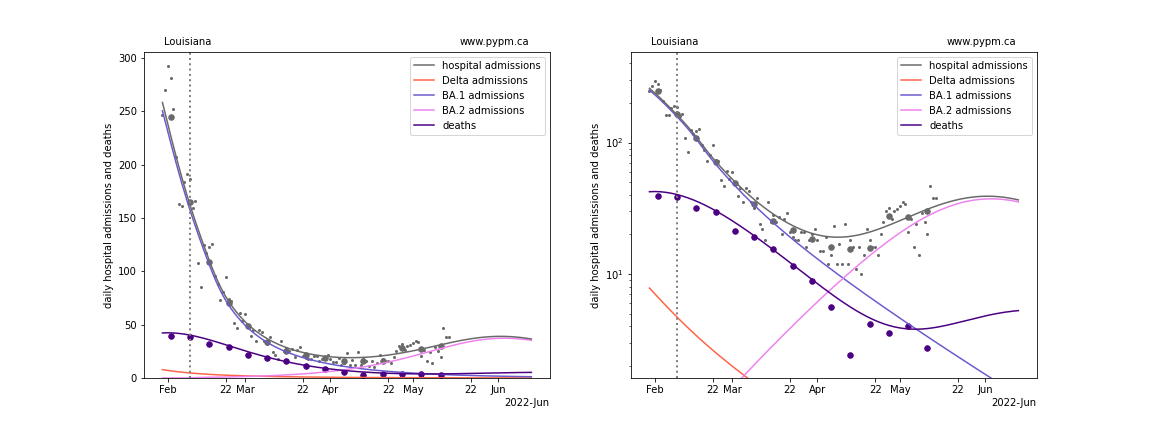
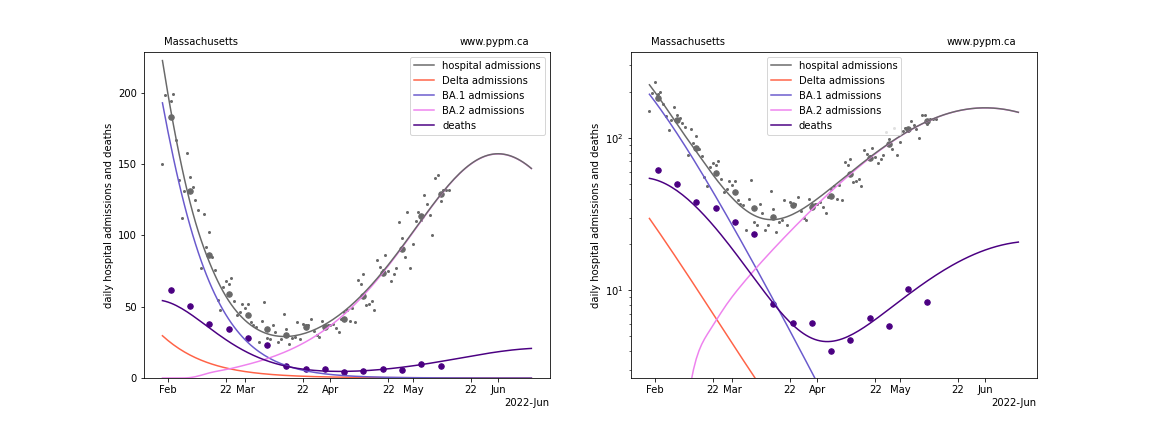
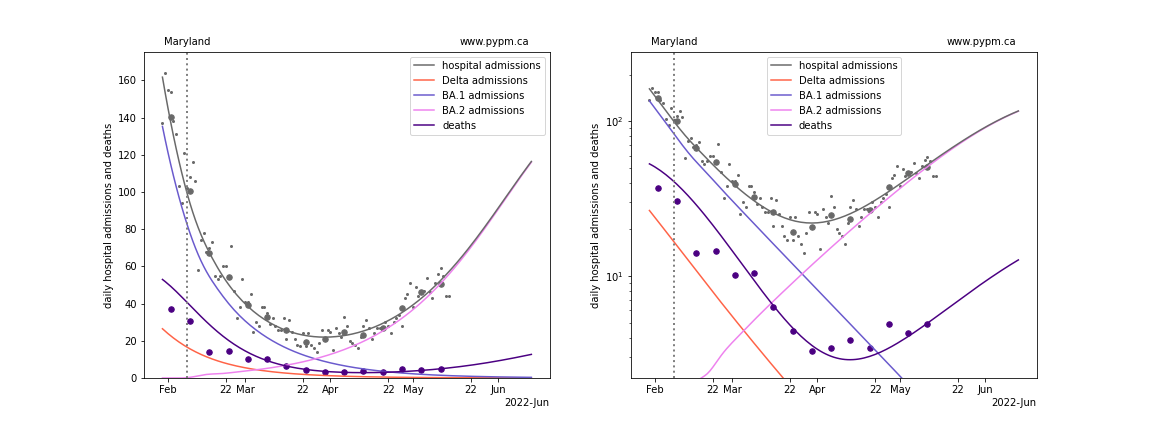
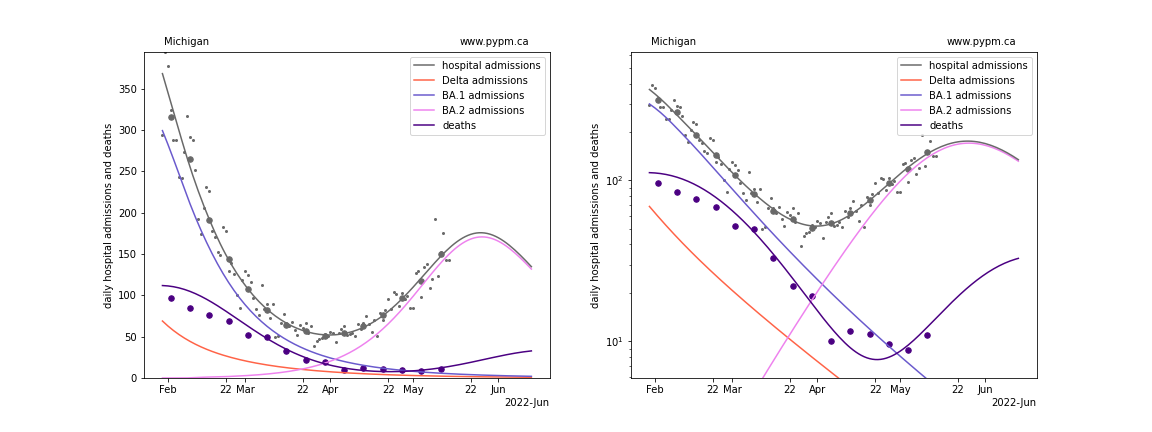
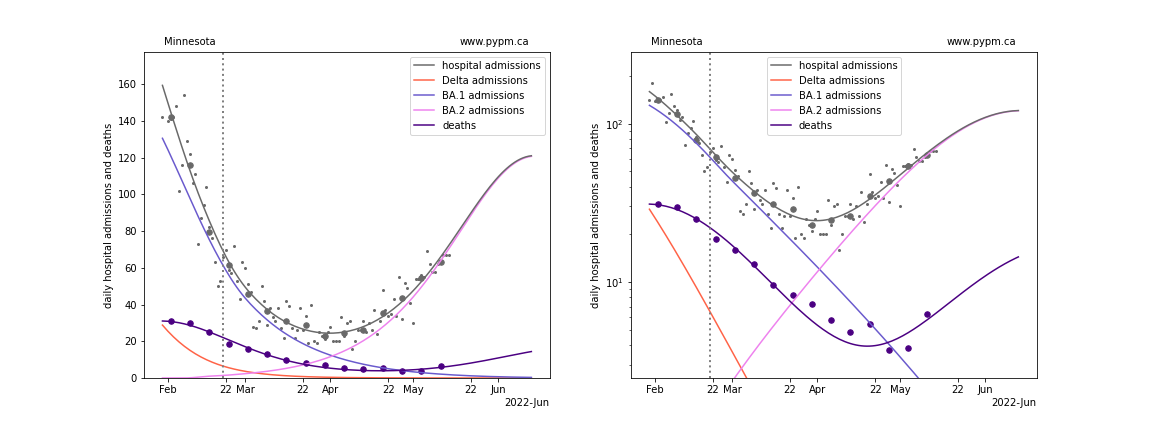
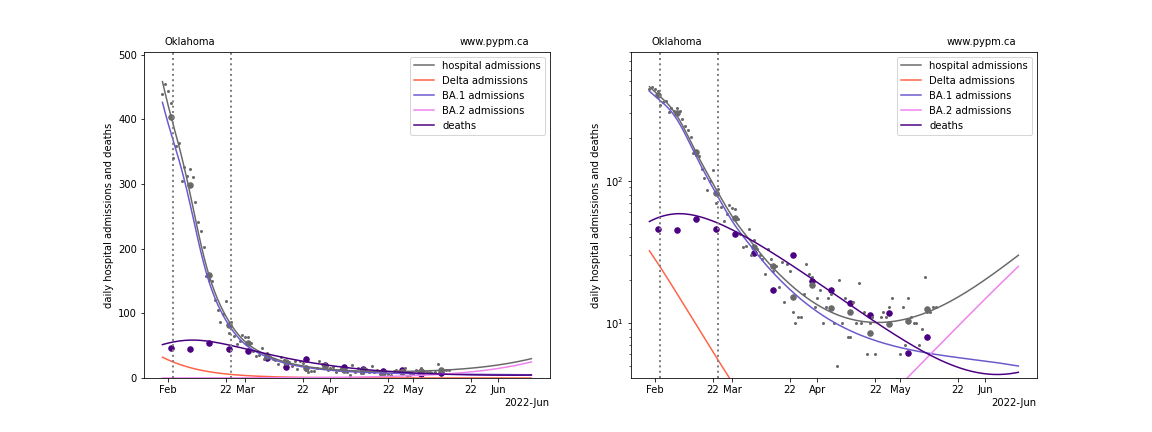
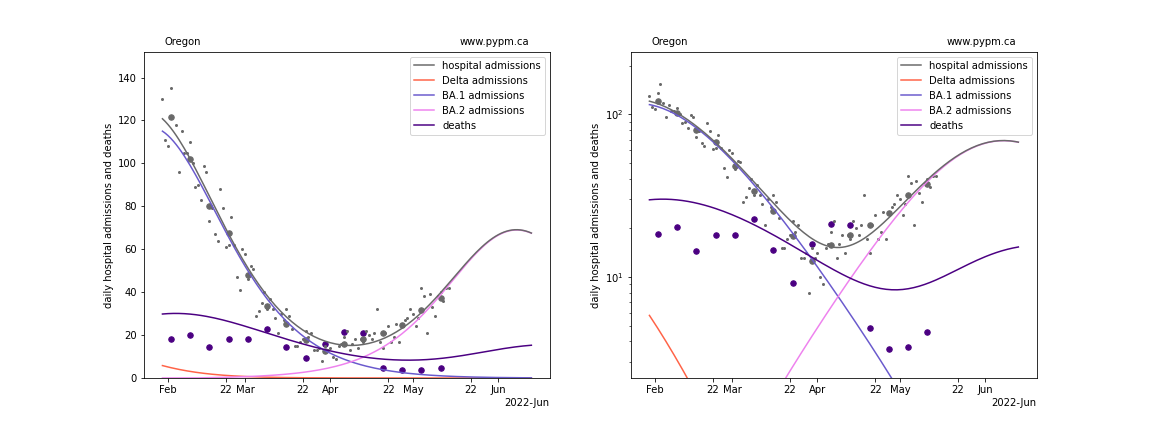
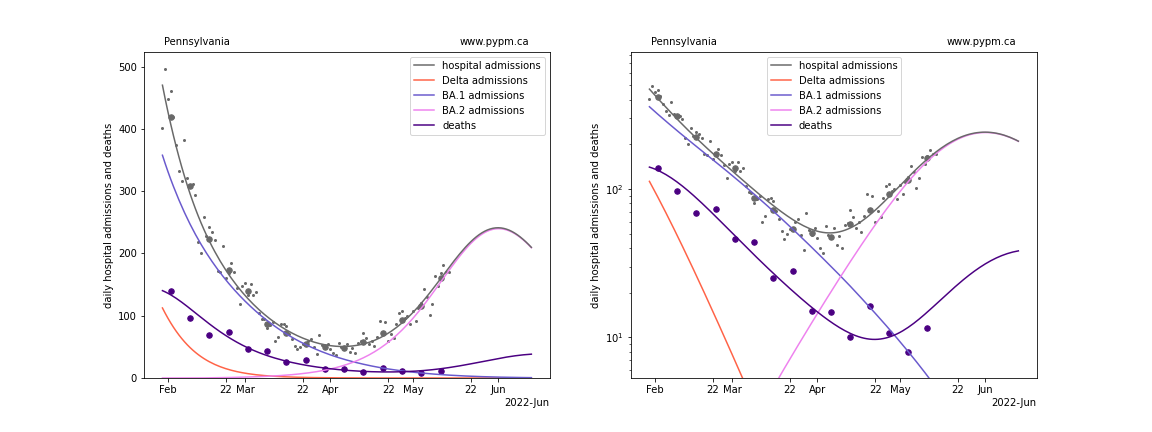
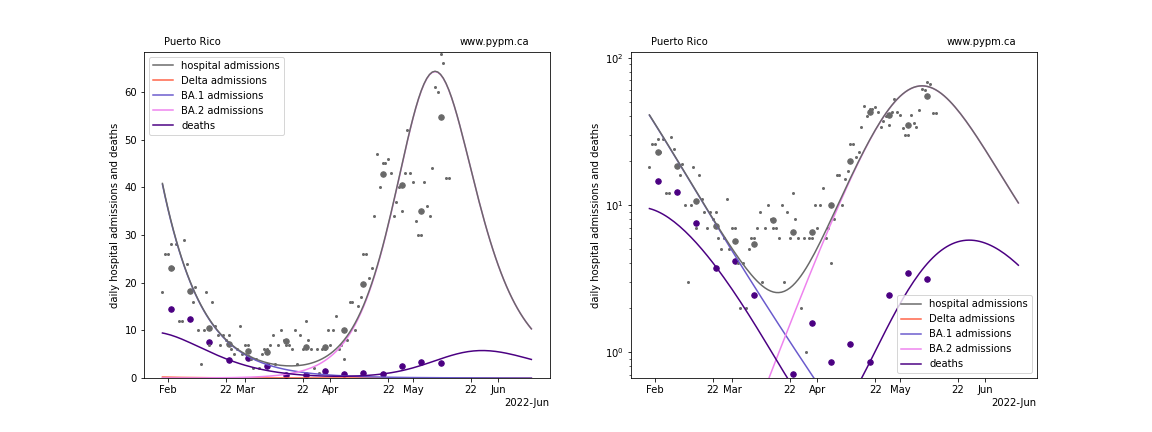
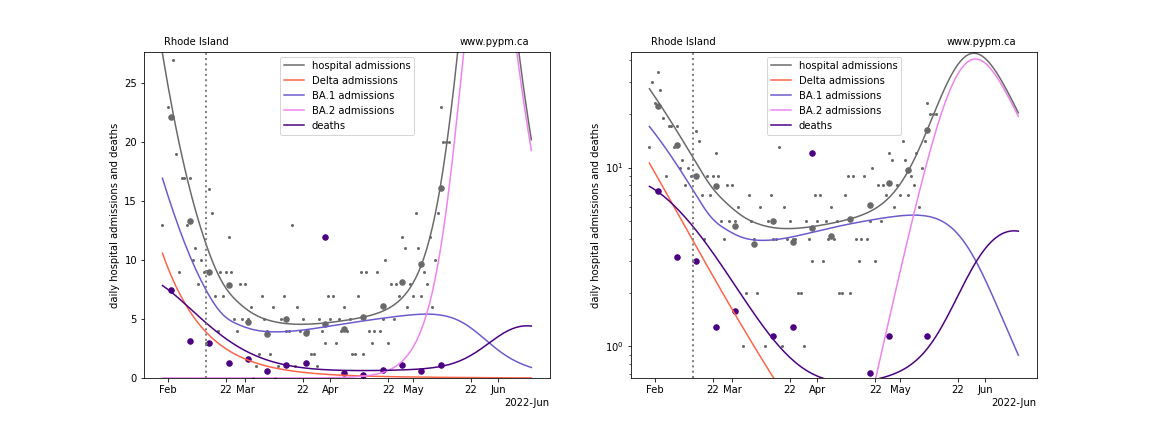
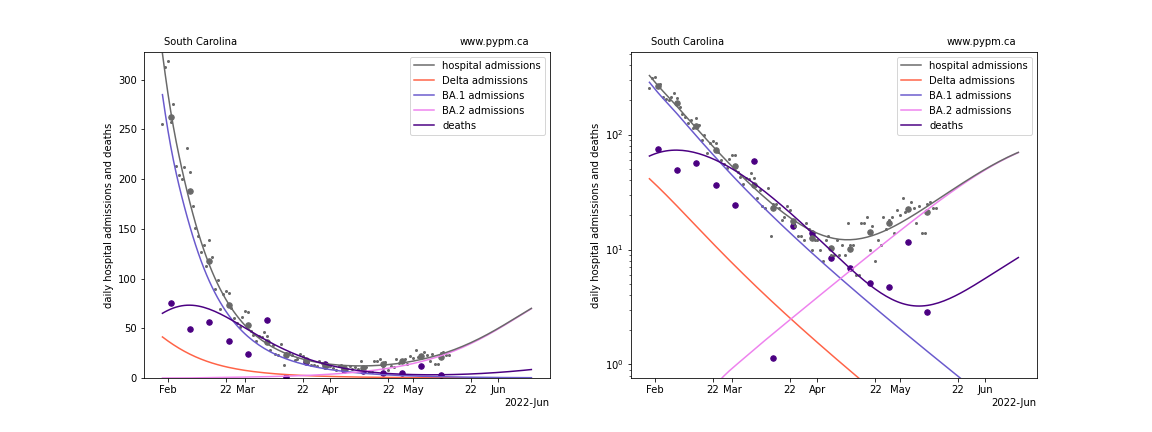
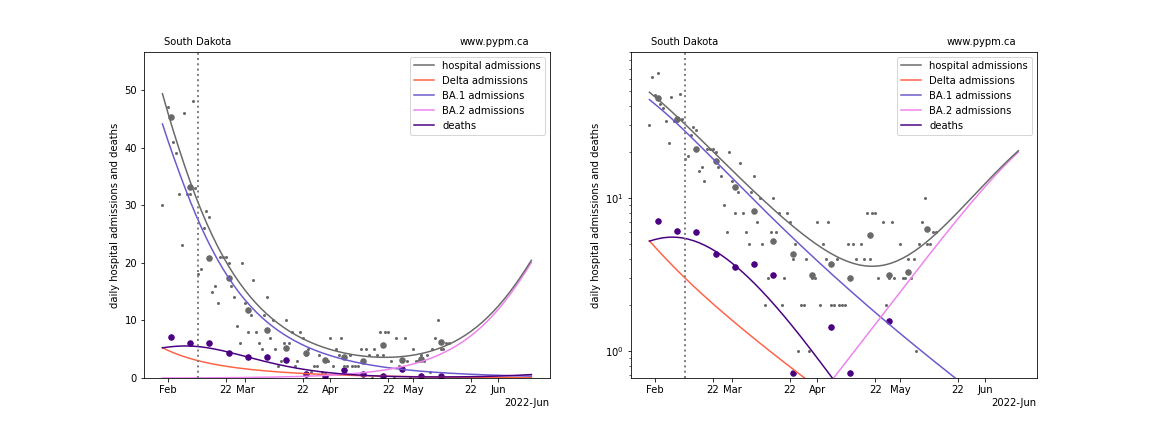
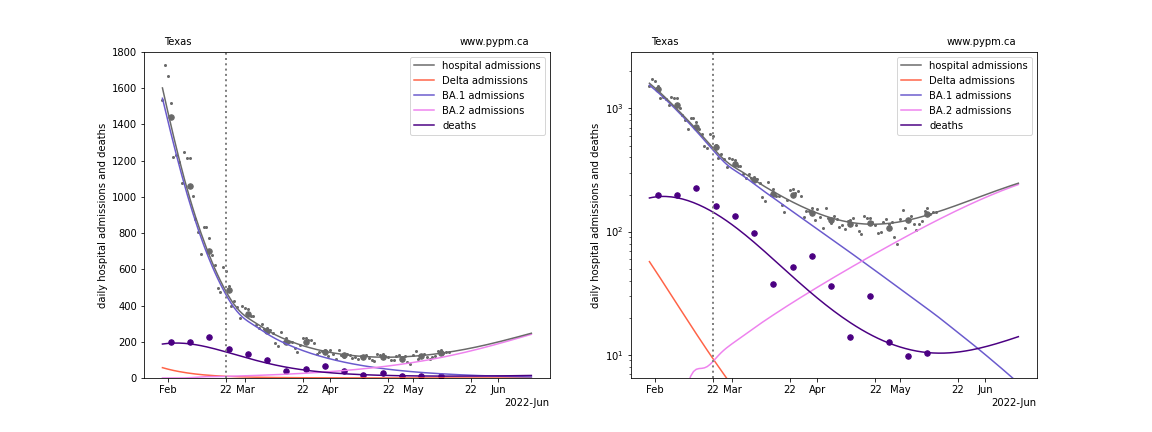
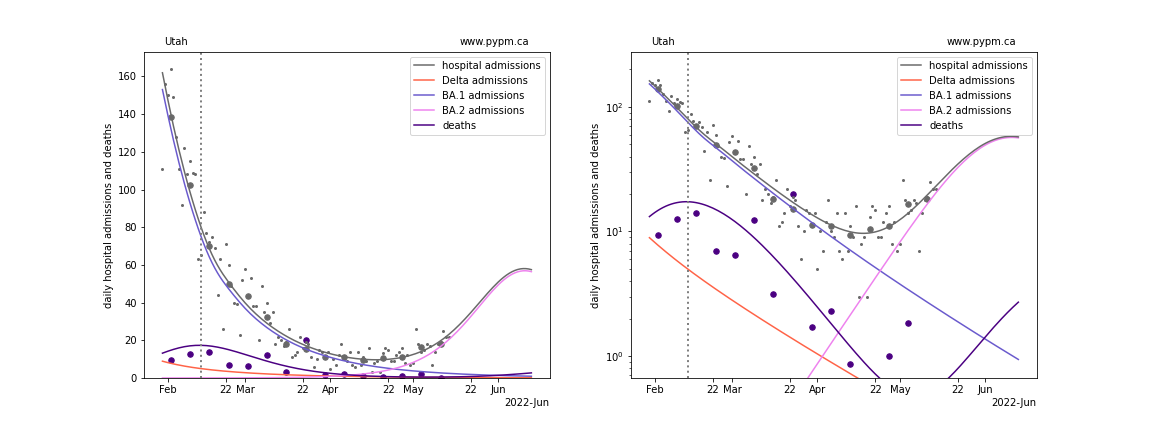
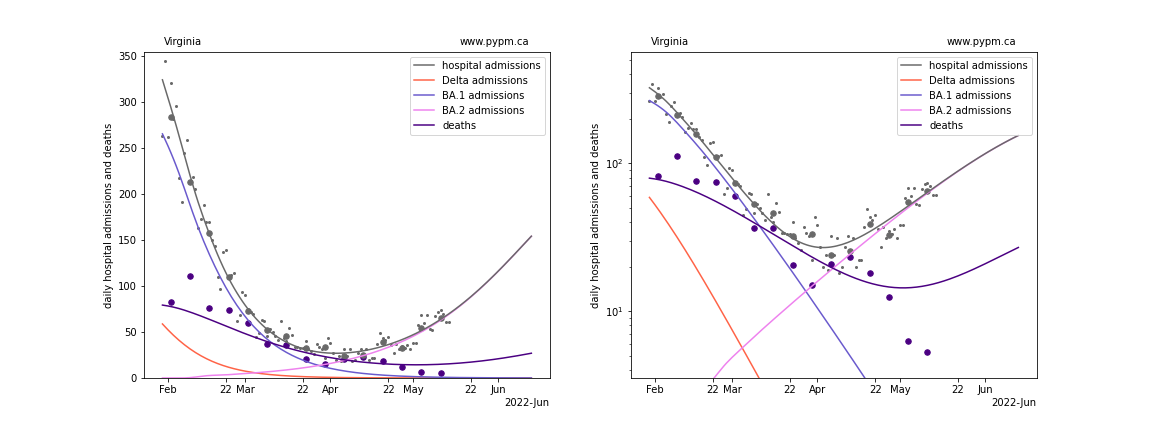
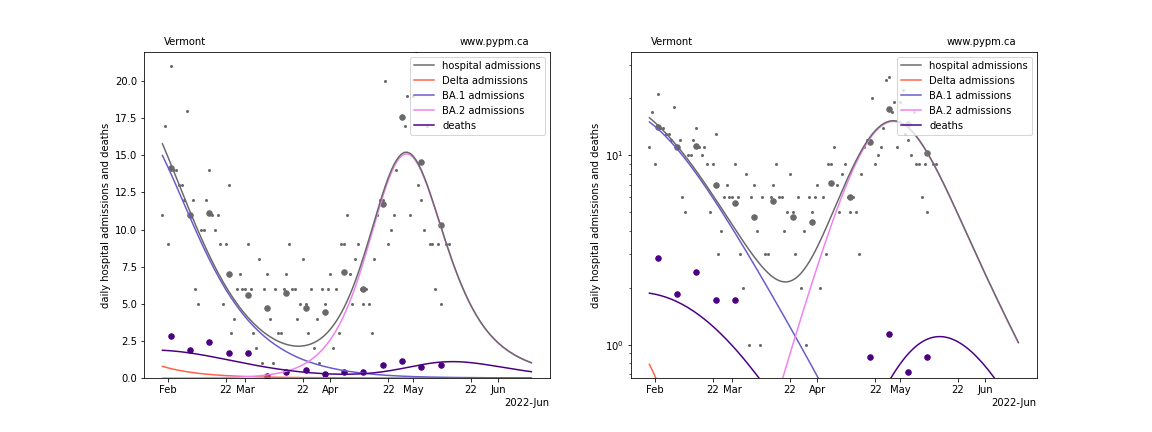
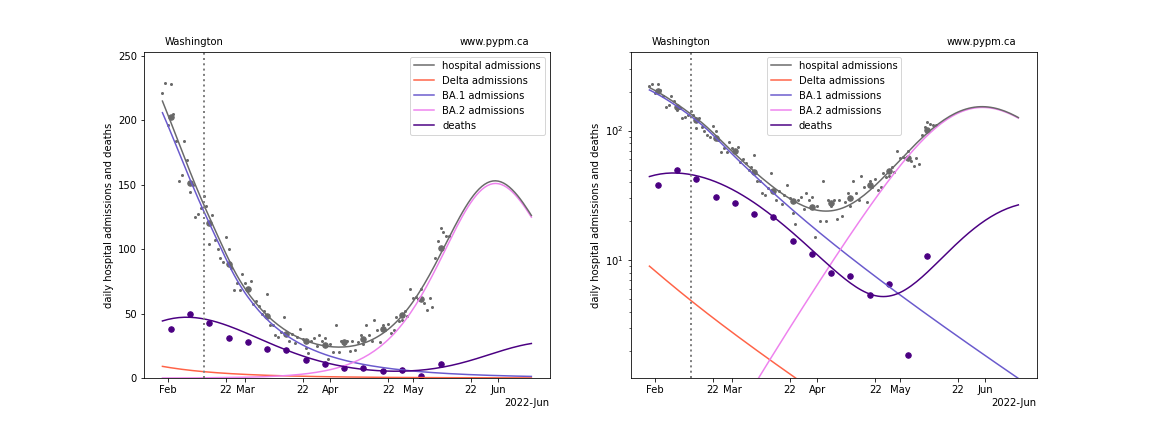
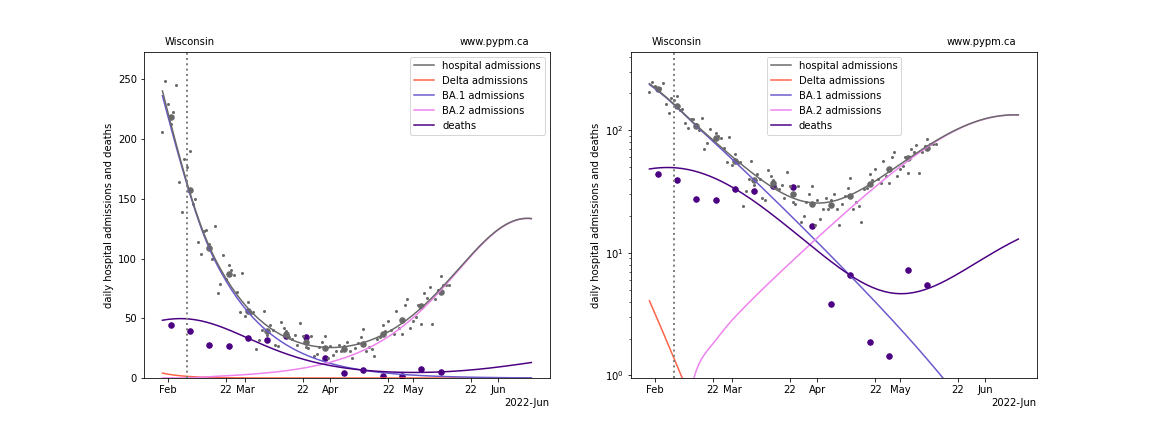
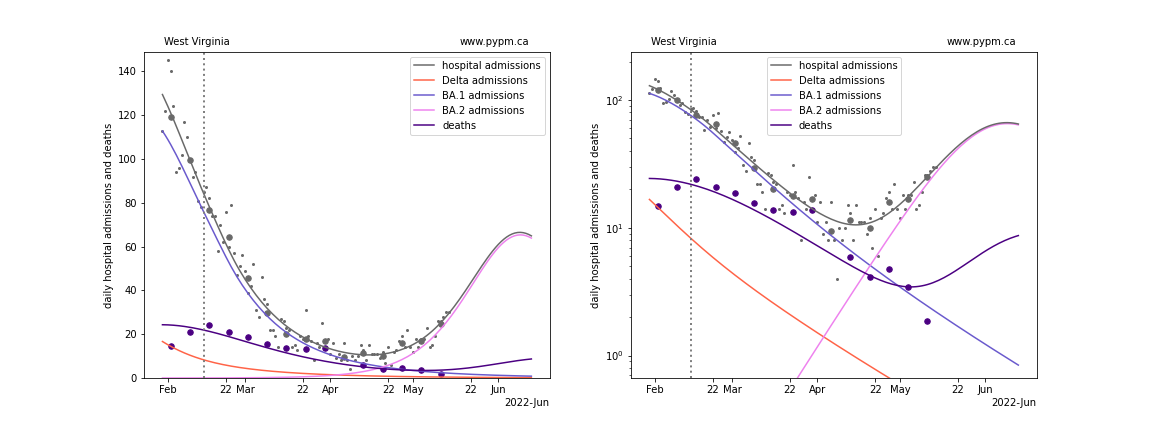
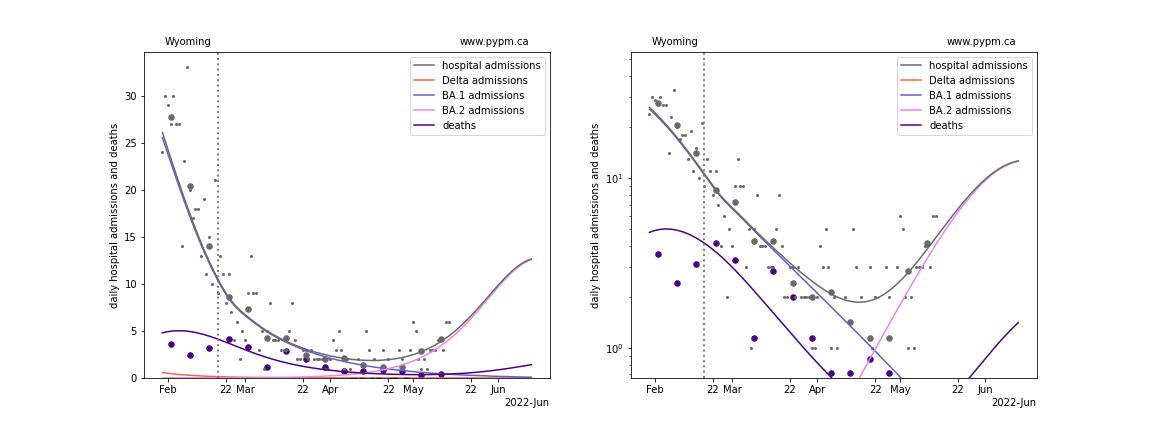
In the figures below, the small dots show daily values, and the larger circles are weekly averages to help guide the eye.
The vertical dashed lines show where the transmission rate is changed in the model to better fit the data. If the susceptible fraction is constant (immunity not changing quickly), constant transmission rates lead to steady exponential growth or decline. With immunity growing, the curves bend downwards due to the herd effect.
With the large number of BA.1 infections providing natural immunity, the model predicts turn-overs in hospital admissions in the coming weeks for many states. There are a number of assumptions made to characterize population immunity and as a result these forecasts have a great deal of uncertainty.
Individual state hospitalization analyses
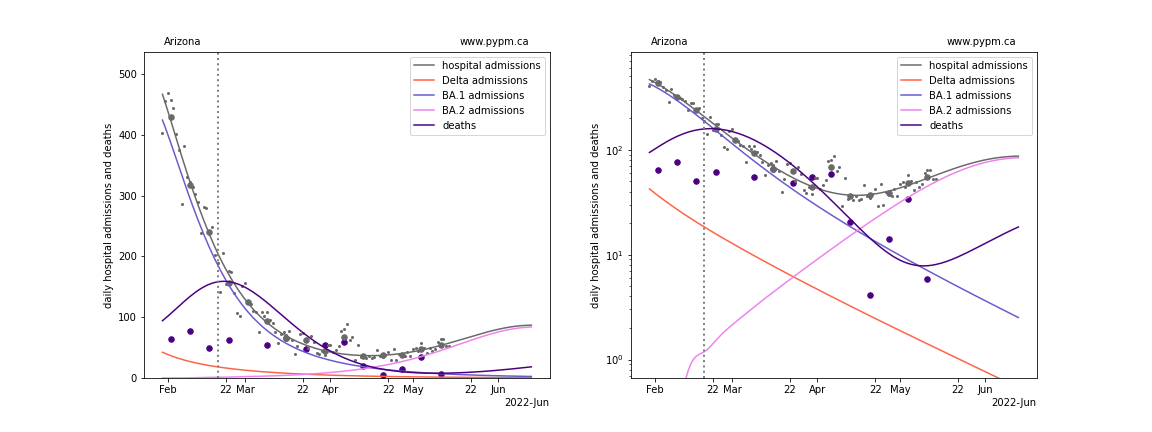
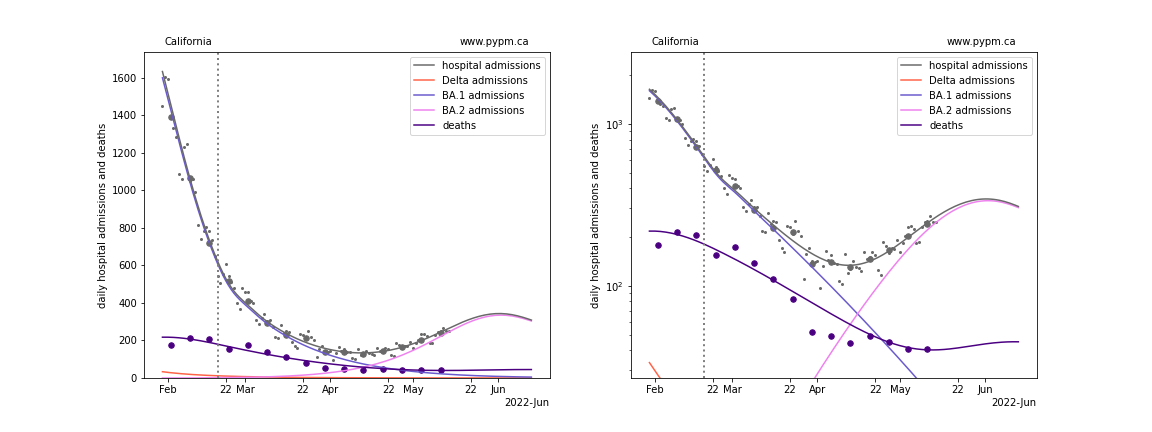
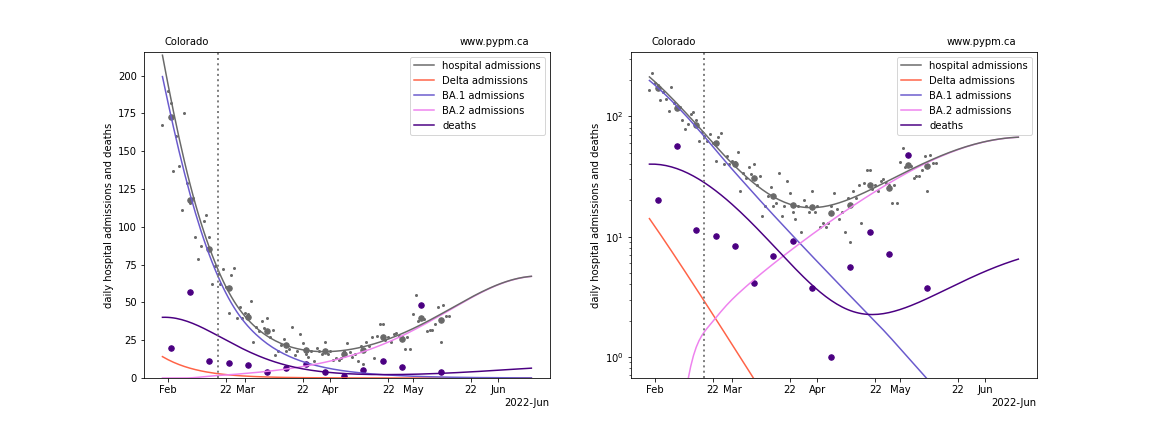
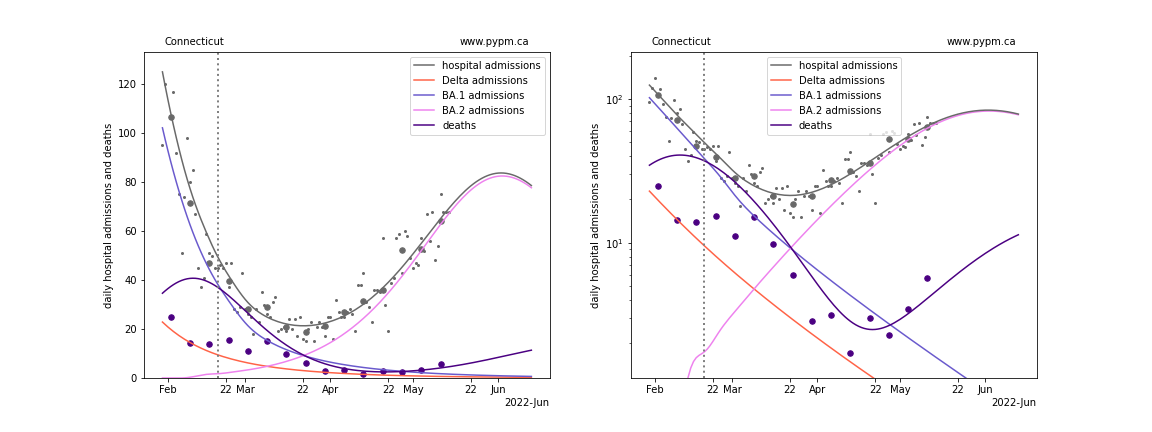
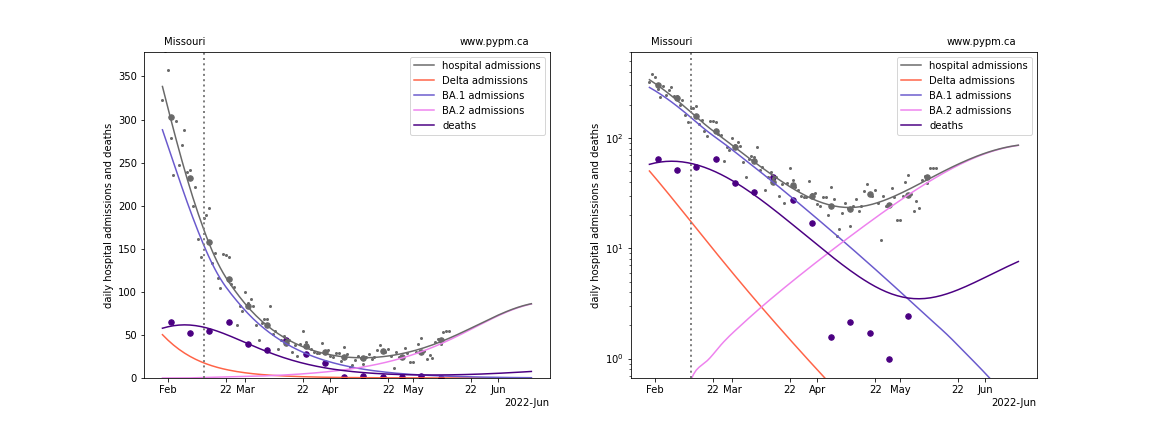
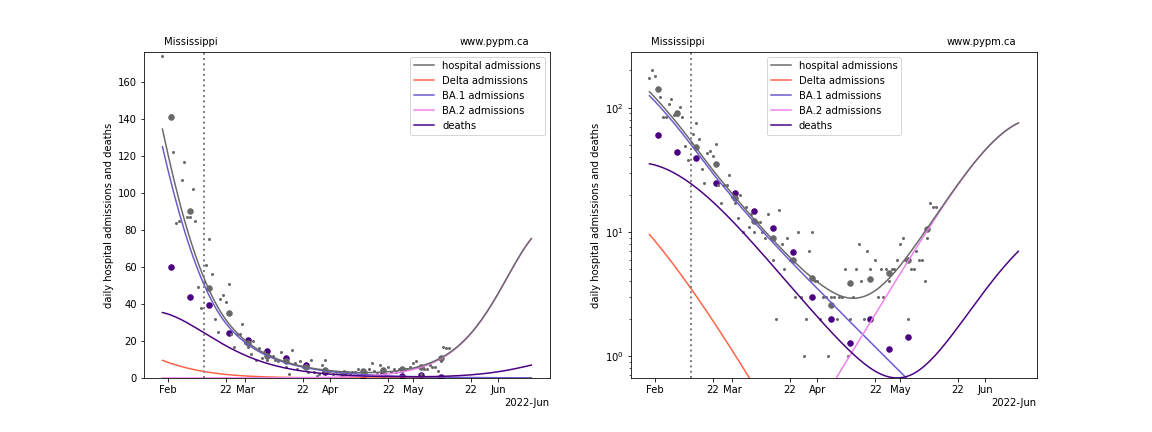
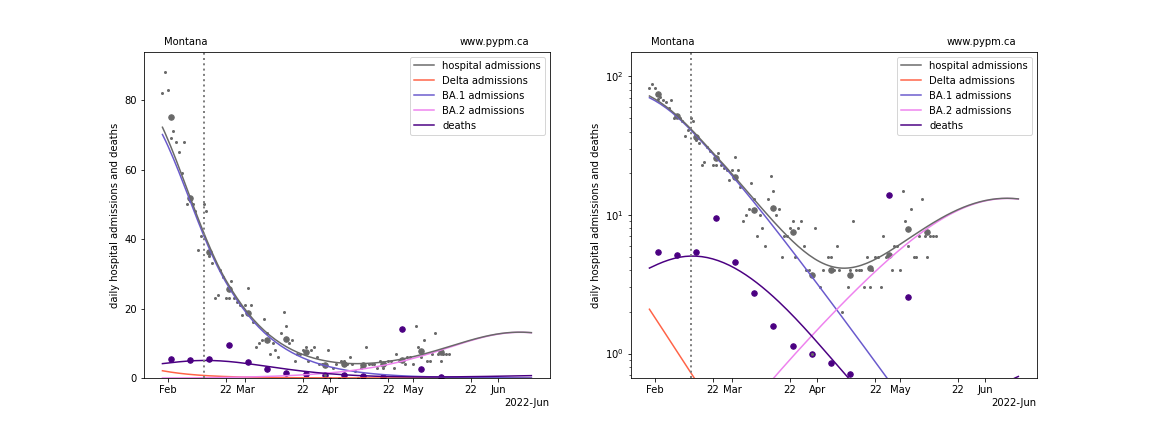
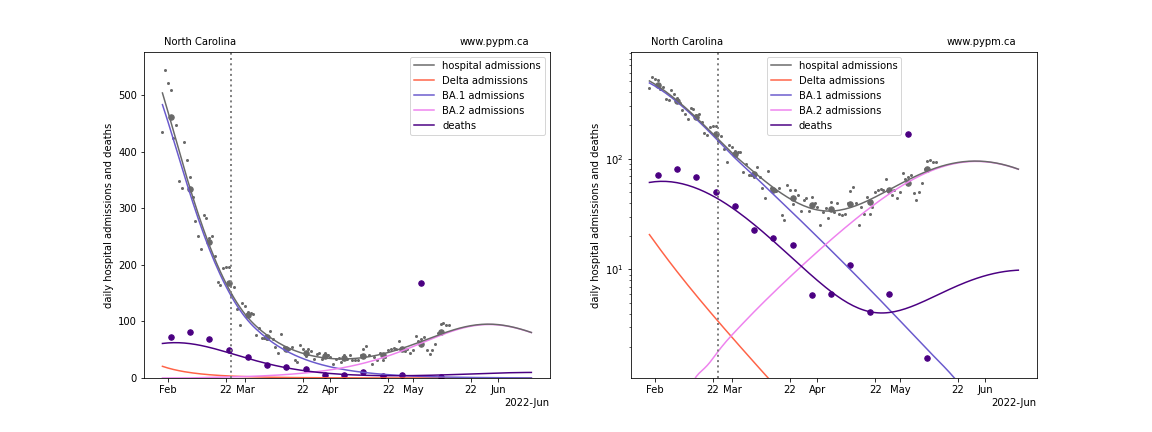
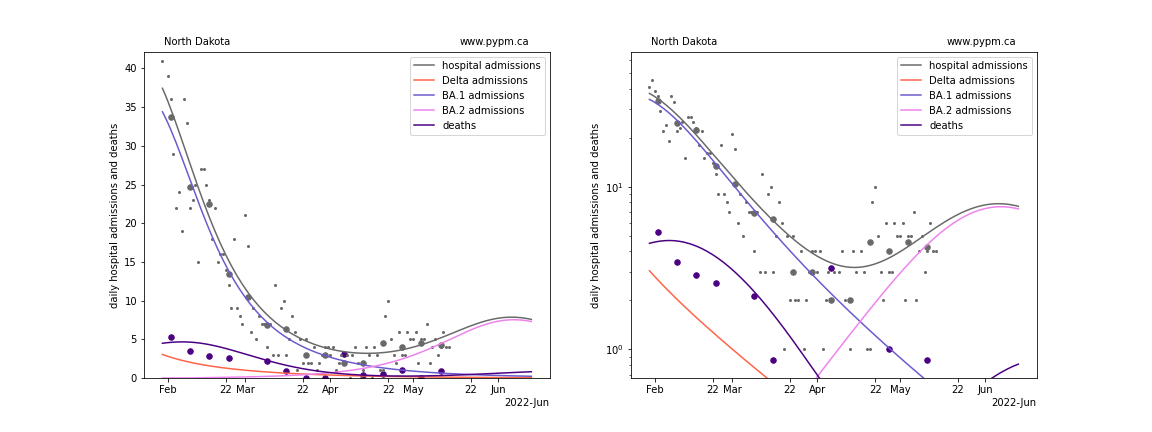
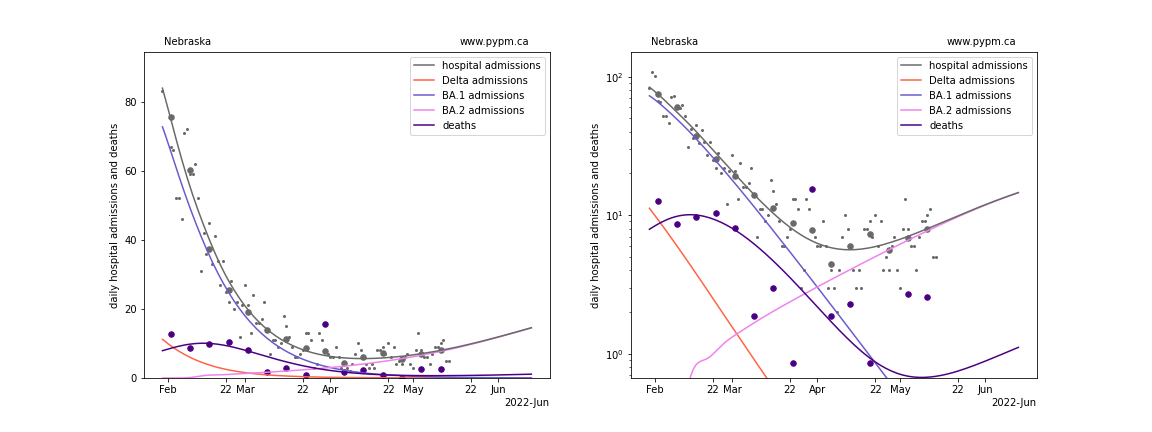
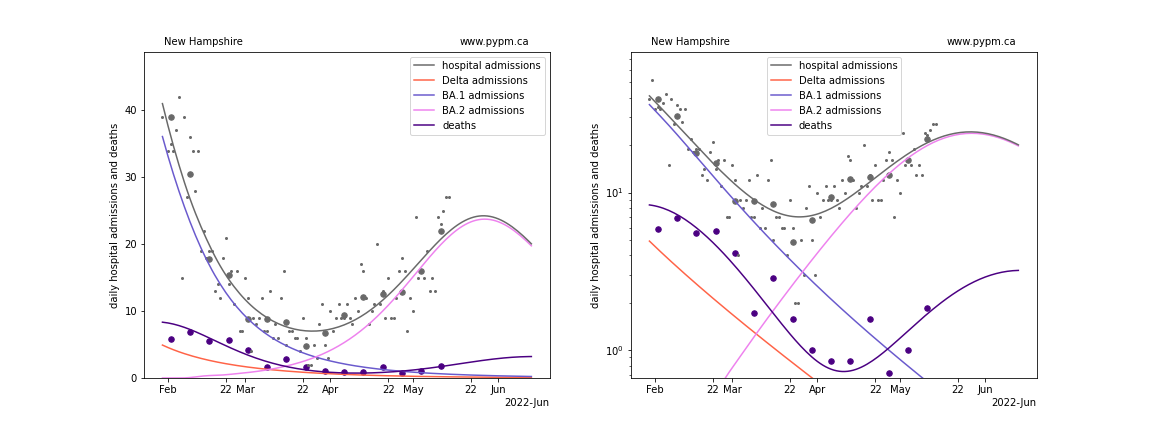
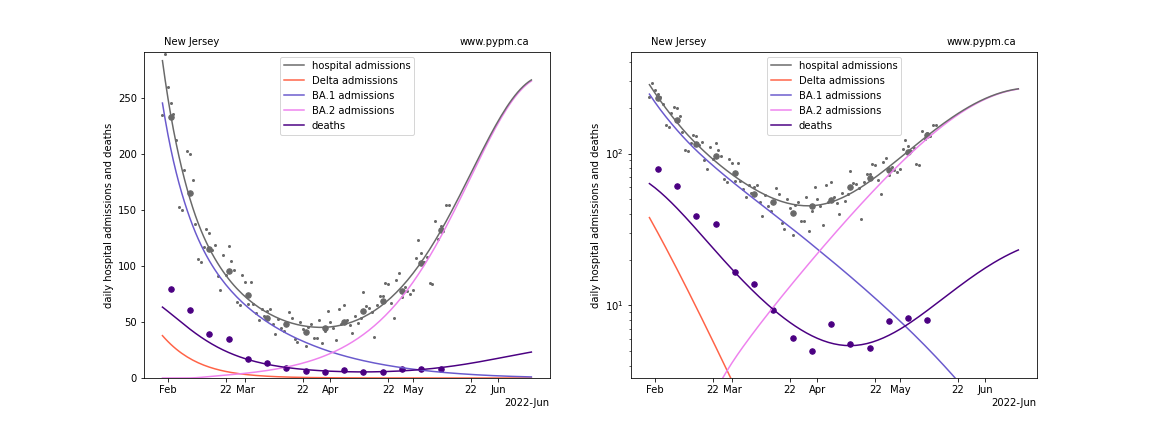
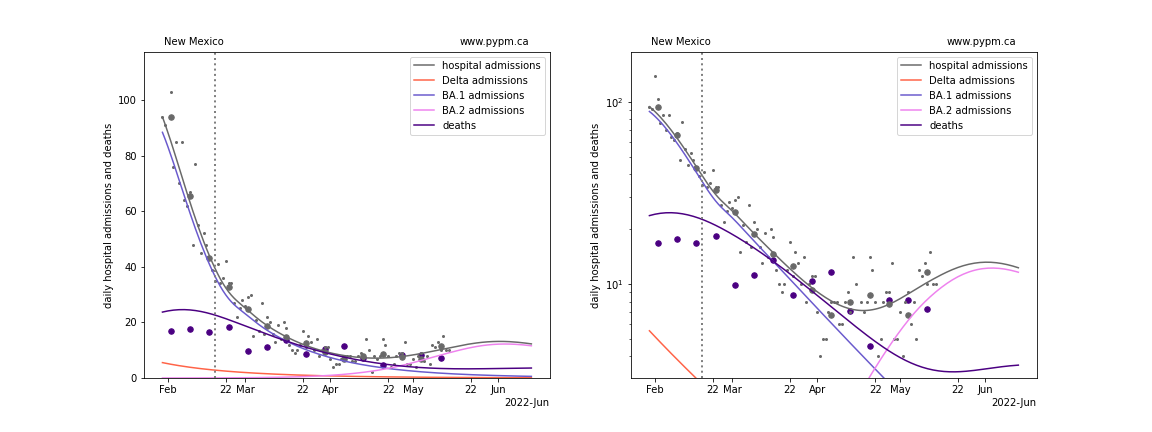
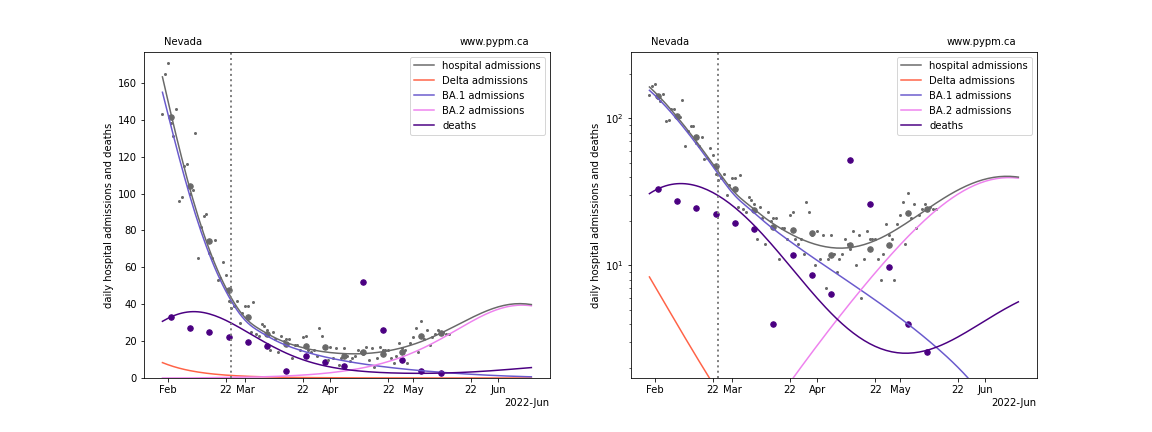
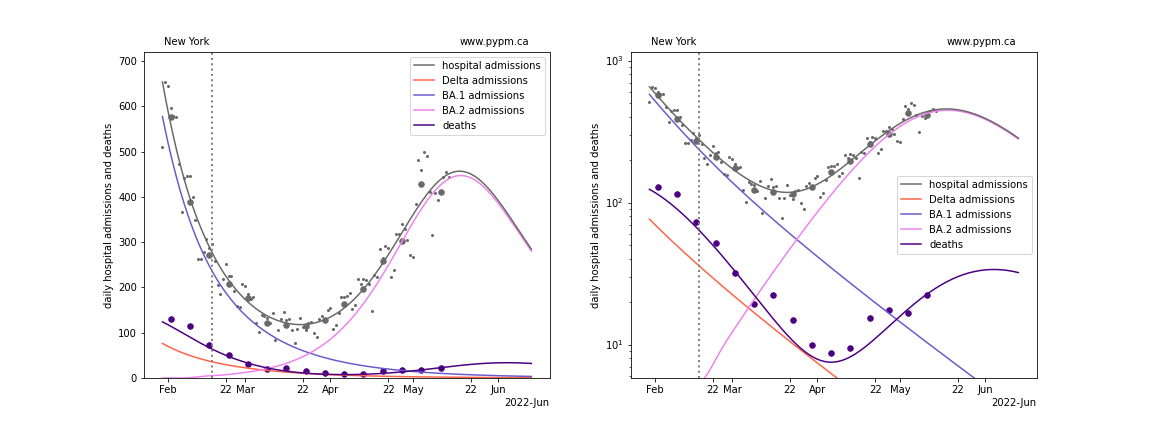
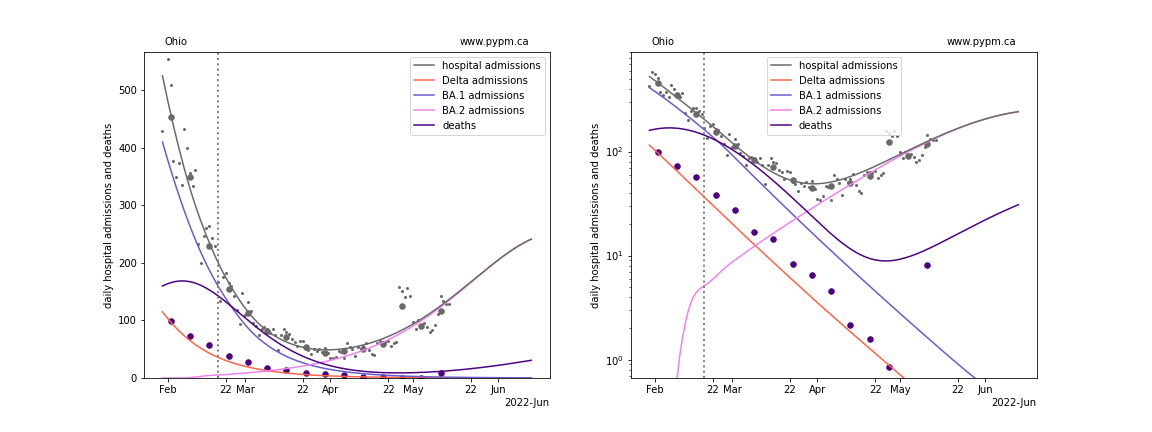
The plots for each state below show the daily hospital admissions and deaths since early February on a linear scale (left) and log scale (right). The figures show how the model attributes admissions from Delta and Omicron infections.
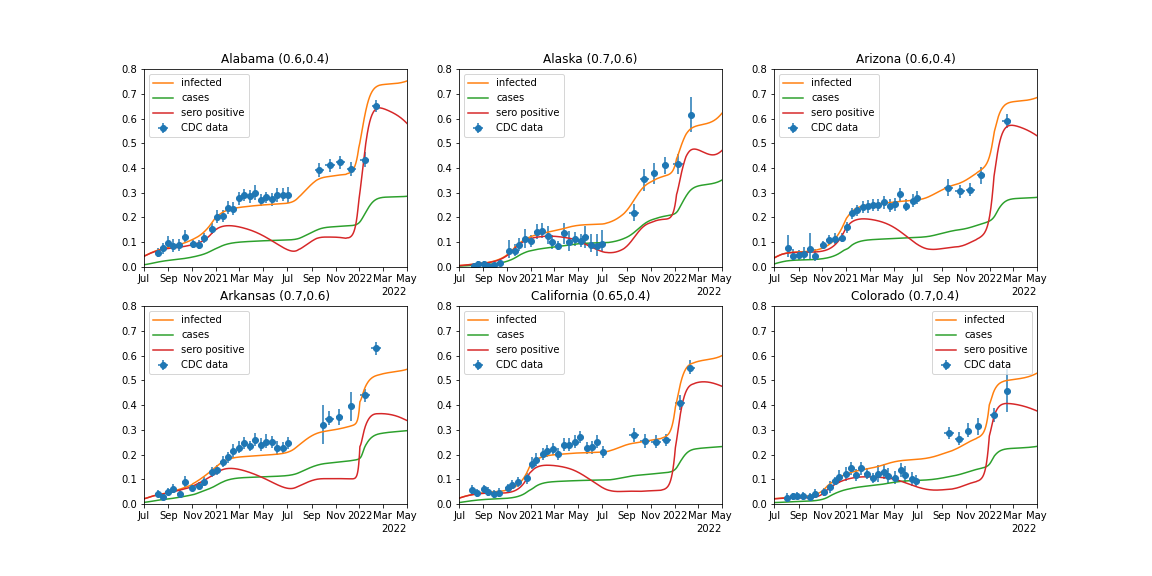
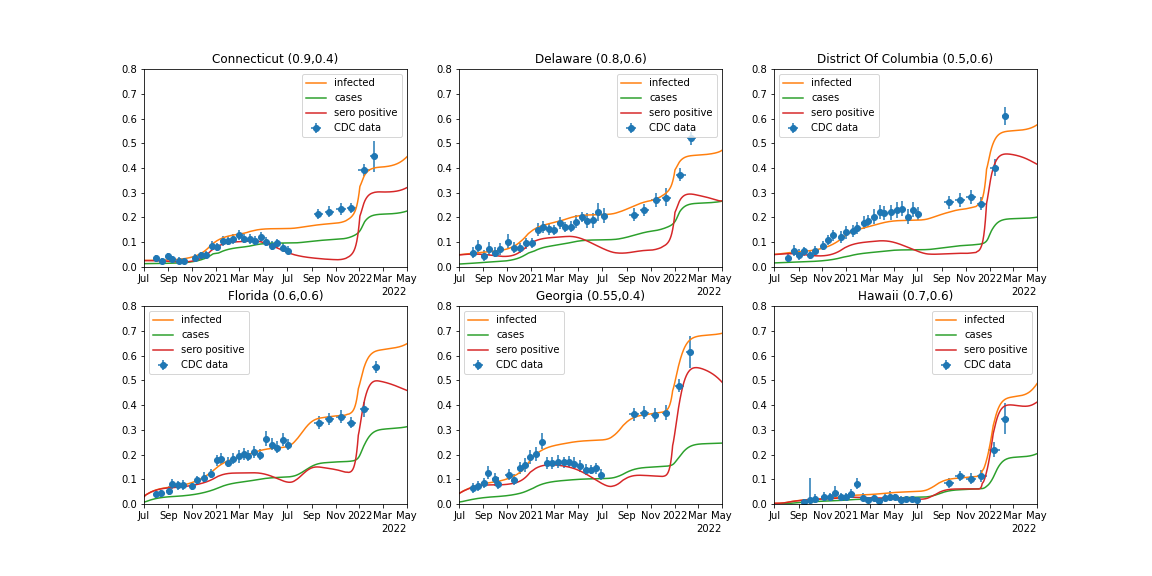
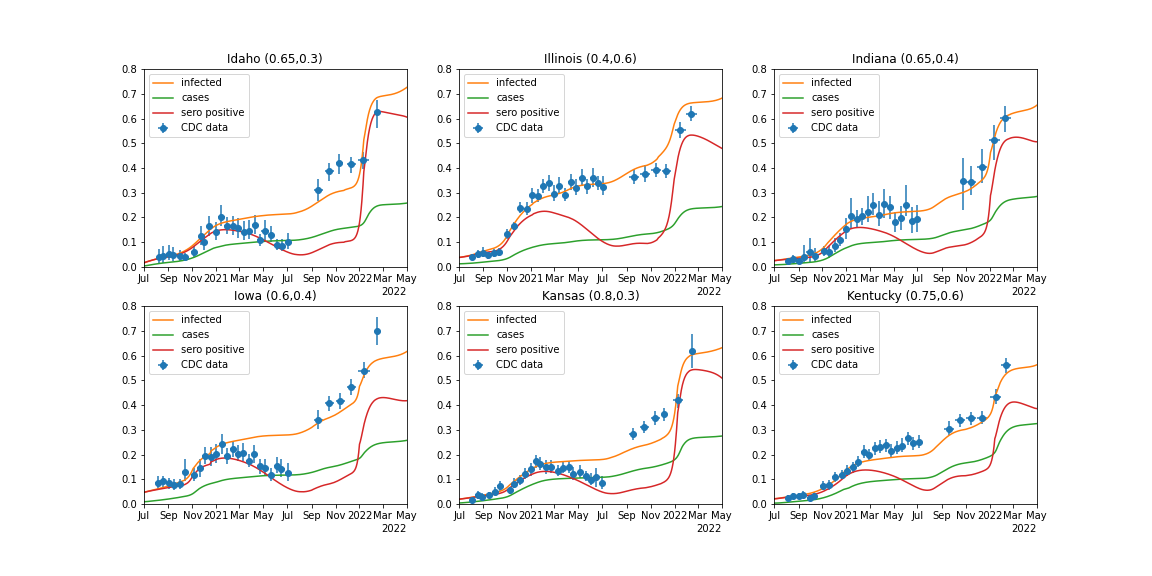
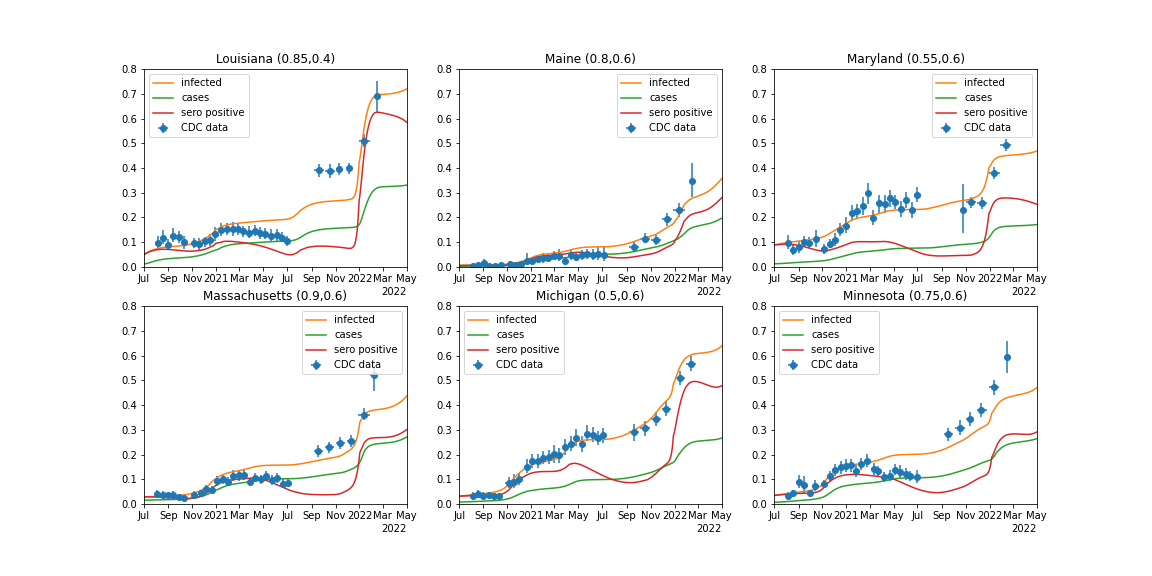
Following the individual state plots, summaries of all states are shown below.
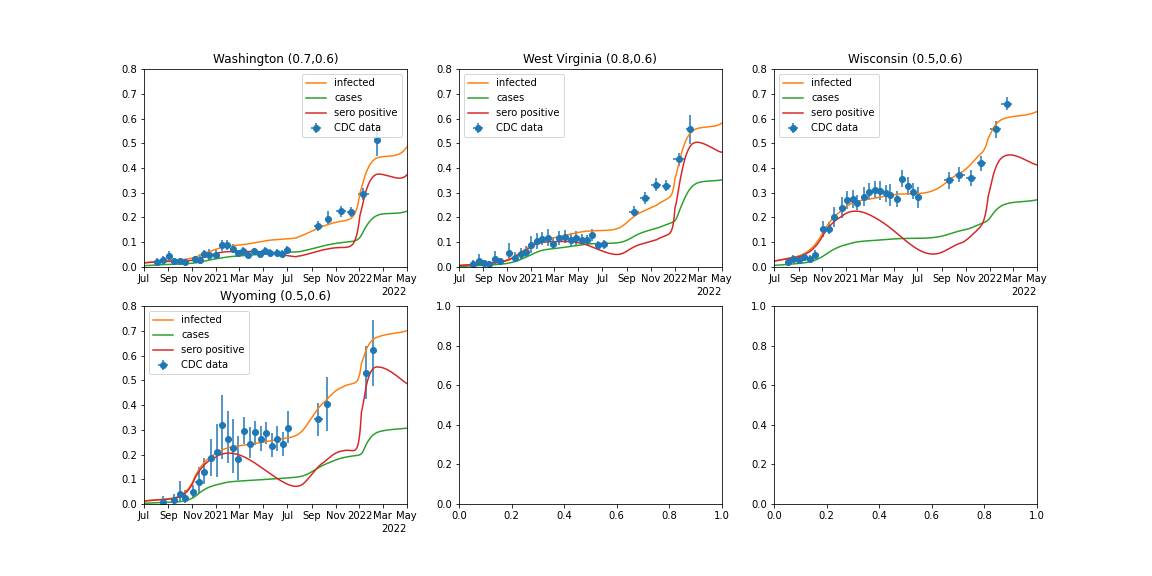
Also shown are seroprevalence data compiled by CDC in comparison to model predictions. Getting the correct number of natural infections is one of many factors in developing a useful immunity model.
Alaska
Alabama
Arkansas
Arizona
California
Colorado
Connecticut
District Of Columbia
Delaware
Florida
Georgia
Hawaii
Iowa
Idaho
Illinois
Indiana
Kansas
Kentucky
Louisiana
Massachusetts
Maryland
Maine

Michigan
Minnesota
Missouri
Mississippi
Montana
North Carolina
North Dakota
Nebraska
New Hampshire
New Jersey
New Mexico
Nevada
New York
Ohio
Oklahoma
Oregon
Pennsylvania
Puerto Rico
Rhode Island
South Carolina
South Dakota
Tennessee

Texas
Utah
Virginia
Vermont
Washington
Wisconsin
West Virginia
Wyoming
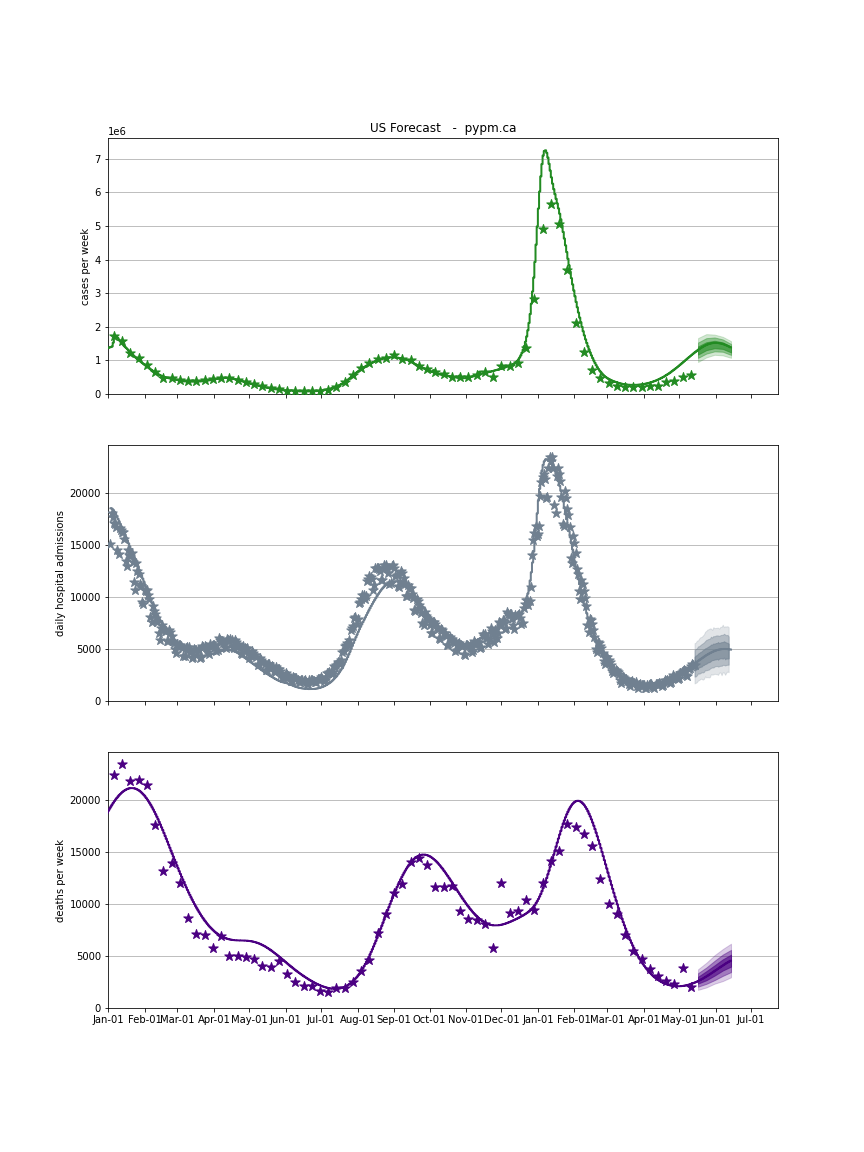
USA Forecast
The following plots show the combined US 4 week forecast. The shaded areas are 50%, 80%, and 95% intervals. The case forecast should be ignored, since the fraction of cases being reported reduced dramatically in early 2022.
USA
Seroprevalence
The US-CDC coordinated a nationwide survey of COVID-19 Infection-Induced Antibody Seroprevalence through commercial laboratories.
The 2020 data were used to estimate the fraction of symptomatic cases that were reported. Prior to Sept 2021, some states used the Abbott Assay whose test sensitivity wanes (50% efficient after 6 months) resulting in reduced seroprevalence. The sero-positive curves show the expected data for that assay (by incorporating the waning of test sensitivity). All states use the Roche Assay after Sept 2021, which is to be compared to the infected curve. For most states, the model seroprevalence is similar to the data.